Population Council Vaccine Study
Rebuttal or Whitewash?
A look at Vaccination in Ghana,
an unsubstantiated and unscientific claim that vaccines save lives
- One study showed the DTP Vaccine was associated with increased death rate of children in Guinea-Bissau.
- A WHO Population Council rebuttal claimed 4 vaccines including DTP were associated with increased survival rates.
- The rebuttal study was conducted in an district where child mortality had been very high. Before various health initiatives were made, approximately one child in four died before age 5 years.
- The study area was characterized by poverty, malnutrition, unclean drinking water, illiteracy and malaria. These conditions have a long history of association with high child mortality rates.
 The wearing of bowler hats is associated with better health.
The wearing of bowler hats is associated with better health. The use of cow manure on gardens is associated with healthier vegetables.
The use of cow manure on gardens is associated with healthier vegetables.
 The use of vaccines (injectable waste material) has been associated with lower mortality. The use of vaccines has
also been associated with higher mortality and multiple modern as well as ancient diseases.
The use of vaccines (injectable waste material) has been associated with lower mortality. The use of vaccines has
also been associated with higher mortality and multiple modern as well as ancient diseases.
Which of these associations are simply temporal, that is events occurring at the same time but without a causal connection and which associations are casually related?
The wearing of bowler hats is not a cause of better health. However, in England, bowler hats were popular in higher society where the advantages of better socio-economic conditions prevailed, such as less strenuous jobs (mine owners not mine workers) and better year around diet that led to better health. Thus the association of bowler hats to health is a correct temporal association but not a causal association.
The use of manure (animal waste) on gardens nourishes the soil and thus the use of manure actually causes healthier vegetables. This is a casual association.
The use of vaccines (injectable waste material) has occurred along side vast improvements in sanitation and nutrition as well as hygiene, better ventilated housing and many other environmental changes. Separating the individual effects of each lifestyle change can be quite challenging, however it is well documented that sanitation and nutrition are the major factors in lowering childhood mortality and controlling infectious diseases.
Our central question is:
Are vaccines associated with lower mortality only as a temporal association, such as the wearing of bowler hats is temporally associated with better health, or is there an actual causal relationship, similar to putting manure on gardens?
This question can be answered with scientific trials, but vaccine proponents are highly reluctant to engage in such tests. Much information to answer this question can be gained from reading a true history of vaccines, as well as comparing the health of vaccinated to non-vaccinated individuals. However, that study is outside the scope of this web page. Please see our Home Page
To understand why we can say that a published pro-vaccine rebuttal to vaccine harm did not follow standard scientific procedures, let us start with an analogy.
An Analogy
 Once upon a time an experimenter entered an area where a large number of children died before their fifth birthday.
The experimenter determined that the mortality rate could be cut in half if most of the children drank a mixture of several
raw vegetables made into juice and combined with small amounts of several poisons. The growers of each vegetable claimed
that their vegetable was the most important one in preventing children's deaths. The manufacturers of each poison associated
their poison with the 50% decline in mortality and claimed their poison was essential to the survival of children everywhere.
Once upon a time an experimenter entered an area where a large number of children died before their fifth birthday.
The experimenter determined that the mortality rate could be cut in half if most of the children drank a mixture of several
raw vegetables made into juice and combined with small amounts of several poisons. The growers of each vegetable claimed
that their vegetable was the most important one in preventing children's deaths. The manufacturers of each poison associated
their poison with the 50% decline in mortality and claimed their poison was essential to the survival of children everywhere.
However, the day came when another scientist found that one of the poisons actually contributed to child mortality and
suggested that the overall
benefit of the vegetable drink would be improved by leaving that poison out.
However, none of the vegetable growers and none of the poison
manufacturers would fund scientific tests to prove the relative value of each ingredient of the drink
so its individual contribution to saving children's lives could be calculated.
Thus the drink continued to be distributed with all its poisons included because it could be shown
that the poisons were "associated with the decline in mortality," even though no causal relationship to mortality decline
for any of the poisons was ever proven.
In our analogy above,
the more juice given - The more lives were saved.

Is it also true,
that the more "poison" given, the more lives were saved? ? ?
Could the poison be left out of the "juice" and save even more lives?
That question will be examined below.
- As mentioned in the opening lines above, in the year 2000, a study was published that showed a higher mortality rate [more deaths] among children in Guinea-Bissau, 1990-96, who received DTP vaccine. The data for this study was republished in 2005 by the British Medical Journal. (1)
- The above study was followed by a World Health Organization (WHO) sponsored rebuttal using data collected on children in Northern Ghana(2) that claimed each vaccine given (BCG, DTP, polio and measles) "was associated with lower mortality" in children under 5 years.
- The Guinea-Bissau study that showed more deaths in the vaccinated is not the first crack in the armor of the vaccine industry. Previously, about 1970, Dr. Archie Kalokerinos(3) found that severely malnourished children frequently died immediately after vaccination. [more]
- On the other end of the socio-economic scale, from 1975 to 1980, Japan raised it's age for vaccination from five months to two years and saved many infants' and young children's lives. During that time period, infant mortality rank for Japan rose from number 17 to number one, the best in the world. [more]
The WHO sponsored Population Council study,
Immunization Status and Child Survival in Rural Ghana
is a retrospective study of the
data collected as follows:(2)
Children born in the Kassena-Nankana District (KND) of the Upper East Region (north) of Ghana
between 1 October 1994 and 31 December 1999.
The study sample population was 17,701 children of which 13,452 were vaccinated and 4,249 (24%) unvaccinated.
Records of an additional 6300 children were not used in the study.
The "vaccinated" had an uncorrected estimated average Under 5 Mortality Rate (U5MR) of 125 per 1000 live births.
The "non vaccinated" sample had an uncorrected estimated U5MR of 246 per 1000 live births.
As we will see below, "vaccinated" and "non vaccinated" are extremely
inaccurate and misleading choices of labels if one is honestly striving for scientific facts.
OR
How vaccination takes credit for the benefits of sanitation and nutrition.
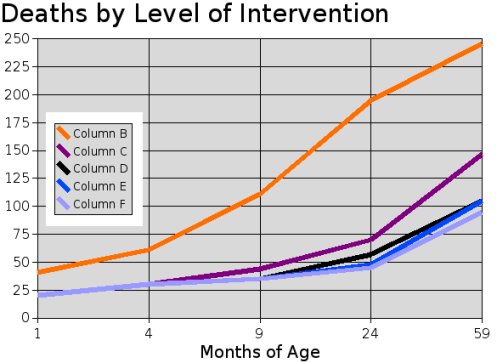
Figure 1.
Figure 1, above, summarizes the claims made by the WHO study authors. Five levels of intervention are shown with the resulting number of deaths per 1000 live births in each group. The column B (red) line shows approximately 246 deaths per 1000 with little or no interventions.
Lines labeled for columns C (Magenta) through F (Violet) show a lower number of deaths associated with higher numbers of interventions (lifestyle changes) including more vaccinations.
Using an estimate for the number of deaths in the first 3 months of life, plus the published data for the 4 to 59 month ages, gives the following total number of deaths per 1000 live births for children under 5 years (U5MR) claimed for each level of intervention:
Estimated U5MRs for children with 5 levels of intervention:
"Unvaccinated" = 246 % Partial series of BCG/polio/DPT = 147 * % Full series of BCG/polio/DPT = 105 * % # Partial series of BCG/polio/DPT and measles = 105 * % # All vaccinations = 95 * % # * Totals do not include an estimate for vaccine caused deaths. % Totals do not include an estimate for deaths in the vaccinated classified as unvaccinated. # No correction for self-selective healthy bias was made.
What is wrong with the above figures?
"Some Juice" = 147 lives lost per 1000 born:
"More Juice" = 105 lives lost per 1000 born:
"Abundant Juice" = 95 lives lost per 1000 born:
-
Major Biases
- The only intervention for which data was given was vaccinations.
- A true "unvaccinated" baseline was not published.
- Deaths in the first 3 months of life were not published.
- Deaths of vaccinated children were sometimes listed as unvaccinated.
- Healthy self selective bias for continuing vaccination after the first in a series of vaccinations is ignored. Bias1 | Interventions | Bias2 | Bias3 | Bias4 | Bias5 | Conclusions
Historically, improvements (interventions) in the areas of sanitation, nutrition and hygiene have been the GREAT immunizers. In the USA. 90% of decline in infectious disease mortality occurred before the introduction in specific vaccines. In certain areas, like Panama, insect control for malaria was also helpful in reducing mortality. In the study area, there were improvements made in all four of these immunizing activities, sanitation, nutrition, hygiene and insect control. Typically, lacks of sanitation, nutrition and hygiene have been associated with poverty. However, no significant economic improvements occurred during the study period. In addition, health promoting lifestyle improvements were not uniformly applied throughout the KND as portions of this district are inaccessible during part of the year.
The large number of non-vaccine interventions that have a high level of efficiency in producing better health and under age five survival rates make it certain that vaccination can NOT be credited with a large part, if any, of the total improvement in mortality in the subject study. Vitamin A capsules alone were credited with a minimum of 20% of the decline in mortality. See the Expanded Background Information.
Yet, going completely against vaccines' proven ineffectiveness, the authors made the absurd claim that "The independent reduction in mortality associated with measles vaccination is 50 percent." This inflated claim is made even while admitting that "a mere 3–4 percent of child deaths can be attributed to measles (Binka et al. 1995)"... Keep in mind that the purpose of the study's unscientific methodology was supposedly to rebut data showing increased deaths in a population of children living in socio-economic conditions similar to the KND area and who had experienced higher mortality in response to the DPT vaccine.
-
A list of interventions into the lifestyle of families in the KND area during the study period includes
sanitation, nutrition, hygiene, education and medical treatment including vaccinations.
- Exclusive breastfeeding increased from 5% to 35% in the study period,
- Insecticide Treated Nets (ITN) to combat malaria,
- iron and folic acid supplements for pregnant women,
- Vitamin A supplement for mothers of newborn babies.
- Vitamin A supplements for children.
- Prenatal and post natal care (basic midwifery),
- antibiotic therapy and,
- family health, nutrition and hygiene practices were taught.
- Provision of curative services for acute respiratory infections, malaria and other ailments,
- improved access to basic health services,
- de-worming,
- Oral Rehydration Therapy,
- other home care for diarrhoea,
- and of course, vaccinations for BCG, Polio, DTP and Measles.
This list of lifestyle changes can be expanded as follows:
Note: The number of Insecticide Treated Nets was low and stable during the study period. Many other educational and medical based interventions increased in the study period due to the posting of community nurses. Of interest is the fact that Measles vaccination coverage declined during this period of improving mortality.
If most of the interventions in the long list above contribute to a decline in child mortality, then one or more of the interventions could actually be harmful and still the total effect of all interventions would be to lower childhood mortality.
"Non Vaccinated"
Wrong label for minimal or NO Interventions
A grossly inflated baseline is used for Unvaccinated Children
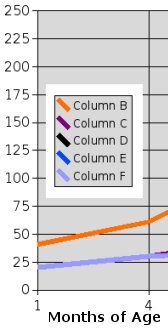 Figure 2 at the right is a subset of Figure 1 and shows mortality rates for only the first four months of life for children
in the KND during the study period.
Note the starting points of the red and blue lines at the lower left side of the chart.
The samples of children labeled "vaccinated" had an estimated neonatal mortality
(deaths in first 28 days following birth) of 20-23 per
thousand and the "non vaccinated" labeled sample
had an estimated neonatal mortality of twice the "vaccinated" although both groups were UNVACCINATED
in the first month of life. [Our estimates based on published declines.] Why do two groups of unvaccinated children
have such a wide disparity in neonatal (first month) survival?
Figure 2 at the right is a subset of Figure 1 and shows mortality rates for only the first four months of life for children
in the KND during the study period.
Note the starting points of the red and blue lines at the lower left side of the chart.
The samples of children labeled "vaccinated" had an estimated neonatal mortality
(deaths in first 28 days following birth) of 20-23 per
thousand and the "non vaccinated" labeled sample
had an estimated neonatal mortality of twice the "vaccinated" although both groups were UNVACCINATED
in the first month of life. [Our estimates based on published declines.] Why do two groups of unvaccinated children
have such a wide disparity in neonatal (first month) survival?
A true comparison between vaccinated and unvaccinated children must compare children whose only difference in lifestyle interventions is vaccinations. One can not legitimately compare children who receive a dozen or more interventions including a few vaccinations with children receiving no interventions and claim that the difference in mortality between the two groups is due to vaccination.
The group of children who benefit from non vaccine interventions, affecting both the child and mother, have about half the rate of deaths in the neonatal period as those children who have little or no interventions.
Thus if the children favored with early life non-vaccine interventions continue to receive no vaccinations, and continue to benefit from non-vaccine interventions, then their under five mortality rate (U5MR) should continue to be about half the mortality of those children with no interventions. Half of 246/1000 is 123/1000. This "estimated true baseline" of 123/1000 U5MR for unvaccinated children is less than the 147/1000 estimated deaths listed for the children (Column C) who received a partial series of BCG, Polio and DPT.
It would require only 18 total unpublished (Bias 3) and falsely labeled deaths (Bias 4) per 1000 life births in the 1-3 month age period to bring the U5MR of columns D and E to equal the estimated "true baseline" of the unvaccinated children.
(Columns D or E | 105 + 18 = 123)
The "suggested" minimum of 10/1000 self selected health bias (Bias 5),
plus the lost card (Bias 4)
and unpublished deaths (Bias 3)
would bring Group F's U5MR equal to the estimated unvaccinated base line of 123 deaths per 1000 live births.
(Column F = 95 +10 + 18 = 123)
The association of vaccines with lower mortality is purely a temporal association.
NO evidence was given for any vaccine to support the idea that vaccination saved lives in the KND area.
The study authors admit that the effects of the DTP vaccine in question was not seperated from the effects of the other vaccines given in the study.
The published mortality rates are consistent with all vaccinations TAKING LIVES while the other lifestyle interventions saved more lives than were taken by vaccination.
The published data very carefully tells us NOTHING ABOUT VACCINE CONTRIBUTION TO MORTALITY as well as the contributions to saving lives of other lifestyle interventions.
The published baseline for unvaccinated children is very misleading in that multiple interventions were ignored. The true baseline for unvaccinated children who received the benefit of multiple changes in lifestyle would have been much lower than the published baseline.
Thus the methodology of the study is not merely flawed but is also fraudulent.
Under the socio-economic conditions of the Kassena-Nankana District:
The published mortality rates for variations in vaccination could be re-phased thusly:
-
Children who received:
- Zero Nutritional/Educational/Medical/Hygiene interventions experienced very high mortality.
- Minimal Nutritional/Educational/Medical/Hygiene interventions experienced medium high mortality.
- Most Nutritional/Educational/Medical/Hygiene interventions experienced low to medium mortality.
- All Nutritional/Educational/Medical/Hygiene interventions experienced low mortality, relative to the general socio-economic conditions of the district.
Given what is known about the history of vaccinations, it is expected that the vaccines contributed nothing to the decline in childhood mortality. See Below. The decline in mortality occurred because of the various changes in lifestyle (interventions) and in spite of the harmful effects of vaccinations.
Trend and causes of neonatal mortality in the Kassena-Nankana district of northern Ghana, 1995-2002.
"Overall, the neonatal mortality rate declined at an average of 2.5 per 1000 live births per year: Down by nearly 50% from 40.9 (95%C.I. 34.1-46.8) in 1995 to 20.5 (95%C.I.17.3-22.7) in 2002.
CONCLUSION: The various health interventions undertaken in this district have had the collateral effect of causing decline in neonatal mortality. Neonatal mortality could be further reduced by preventing and treating neonatal infections, having skilled attendance at delivery and the elimination of infanticide." (4)
Vitamin A supplements are credited with 20 to 25 percent of all cause decline in mortality.(4)
Vitamin A supplements may be responsible for a larger percentage, even most, of the all cause reduction in mortality. (5)
Improved diets clearly lower mortality and even an increase in households with non-dirt floors may be beneficial.
The Community Health and Family Planning Project from 1995 to 2004 includes the period of the study above.
Community-based interventional studies have invariably been accompanied by numerous health education campaigns, including improved access to basic health services, high levels of antenatal attendance, use of impregnated bed-nets, etc.(6)
"Posting nurses to community locations reduced childhood mortality rates by over half in 3 years..." (7)
Other services which increased in the study time period were the provision of curative services for acute respiratory infections, malaria and other ailments. (8)
Not already mentioned immediately above are de-worming, Oral Rehydration Therapy, other home care for diarrhoea, exclusive breast feeding and complementary feeding. Preventative treatment of malaria during pregnancy, iron and folic acid supplementation and the use of Insecticide Treated Nets for pregnant women. Care for diarrhoeal diseases, antibiotic therapy and basic midwifery. Family health, nutrition and hygiene practices were taught.
"It was observed that while trends in other regions of comparable geographical, social and economic indicators were either increasing or remained the same that of UER [Upper East Region includes KND] had actually showed positive decline. Between the two five [year] periods (1994-1998 and 1999-2003) Under five mortality rate dropped significantly from 155 per 1000 live births to 79 per 1000 in Upper East Region while increasing in an adjacent region with similar socio-economic conditions. Similarly infant mortality dropped from 83 per 1000 live births to 33 per 1000 live births." (9)
A good background for vaccination studies in developing countries is the story of Dr. Archie Kalokerinos in Australia about 1970. In Dr Kalokerinos experience with children living with marginal nutrition, an intensive vaccination campaign doubled the mortality rate and in one area caused the death rate to go up to 500 per 1000 children, thus the title of the book, "Every Second Child".(3)
While it is understandable that many children who are malnourished will have severe reactions and even die from vaccination, children on the opposite end of the economic scale also benefit from not being vaccinated. Progress in Japan in lowering the infant death rate came nearly to a halt between 1970 and 1973. Less vaccinations in 1974 and 1975 were associated with a decline in infant deaths. From 1975 to 1980 in Japan vaccination was preformed only on children over 24 months of age and Japan's infant mortality continued to decline very rapidly. See: http://www.vaclib.org/basic/japanusa.htm
For a background information on vaccines NOT saving lives see:
http://www.vaclib.org/legal/letters.htm#600
Introduction to sanitation, nutrition and vaccination:
http://www.vaclib.org/intro/present/index.htm
Index page of links to graphs proving vaccination did not save us:
http://www.vaclib/links/graphs.htm
UNIVERSAL IMMUNIZATION Medical Miracle or Masterful Mirage
By Dr. Raymond Obomsawin
http://www.alternative-doctor.com/vaccination/obomsawin.html
Principles of Natural/Alternative Health
Why Vaccines are ineffective
Method of treatment for children
Seeking An Alternative by Ian Sinclair
See also: http://www.vaclib.org/intro/debate5.htm
The flu vaccine does NOT save lives. See: http://www.vaclib.org/basic/fluindex.htm
Polio
http://www.vaclib.org/basic/polio.htm
Some interesting Notes
http://www.idrc.ca/en/ev-43032-201-1-DO_TOPIC.html
Chapter 22. NAVRONGO DSS, GHANA
The field data collection and processing are mainly supported by funds from the Rockefeller Foundation,
with technical assistance from the Population Council. Data are used to compile reports for the
Ghana Ministry of Health, which is the major consumer of the Navrongo DSS data.
http://www.newswithviews.com/Cuddy/dennis84.htm
31) December 1980---Archbishop Peter Proeku Dery of Ghana reveals that "the World Bank denied loans to Ghana until
my country agreed to institute a nationwide contraception and family planning policy. There was also pressure to
legalize abortion, although the Church and the people have so far been able to prevent this. For how long,
I don't know. The World Bank's attitude shows a total disregard for the beliefs of the people of the
Third World." Some years later, Kofi Annan of Ghana will receive the approval of the power elite to
become U.N. Secretary-General, and he will do nothing to stop the slaughter of hundreds of thousands of Rwandans.
http://www.thinktwice.com/birthcon.htm
The Anti-Fertility Gang
Allied with the WHO in the development of an anti-fertility vaccine (AFV) using hCG with tetanus and other carriers have been UNFPA, the UN Development Programme (UNDP), the World Bank, the Population Council, the Rockefeller Foundation, the All India Institute of Medical Sciences, and a number of universities, including Uppsala, Helsinki, and Ohio State.(5) The U.S. National Institute of Child Health and Human Development (part of NIH) was the supplier of the hCG hormone in some of the AFV experiments.(6)
The WHO begain its "Special Programme" in human reproduction in 1972, and by 1993 had spent more than $356 million
on "reproductive health" research.(7) It is this "Programme" which has pioneered the development of the
abortificant vaccine. Over $90 million of this Programme's funds were contributed by Sweden; Great Britain
donated more than $52 million, while Norway, Denmark and Germany kicked in for $41 million , $27 million,
and $12 million, respectively. The U.S., thanks to the cut-off of such funding during the
Reagan-Bush administrations, has contributed "only" $5.7 million, including a new payment
in 1993 by the Clinton administration of $2.5 million. Other major contibutors to the WHO
Programme include UNFPA, $61 million; the World Bank, $15.5 million; the Rockefeller Foundation,
$2.5 million; the Ford Foundation,
over $1 million; and the IDRC (International Research and Development Centre of Canada), $716.5 thousand.
IDRC Books free online
INTERNATIONAL DEVELOPMENT RESEARCH CENTRE
POPULATION AND HEALTH IN DEVELOPING COUNTRIES
Population, Health, and Survival at INDEPTH Sites
Chapters and/or individual countries may be found here:
http://www.idrc.ca/en/ev-9435-201-1-DO_TOPIC.html
Down load this open E book:
POPULATION AND HEALTH IN DEVELOPING COUNTRIES [17 Megabytes - Large download!] http://www.idrc.ca/openebooks/948-8/
References:
(1) Data may be found in a 2005 study published by the British Medical Journal:
DTP in low income countries: improved child survival or survival bias?
http://www.bmj.com/cgi/content/full/330/7495/845-a
For data, see Table 1 in above BMJ article:
http://www.bmj.com/cgi/content/full/330/7495/845-a/TBL1
(2) Immunization Status and Child Survival in Rural Ghana
Abstract: http://www.popcouncil.org/publications/wp/prd/147.html
Full Study: http://www.popcouncil.org/pdfs/wp/147.pdf
(3) Every Second Child by Dr. Archie Kalokerions and Scientist Dr. Glen Detman. See also: whale.to/b/pauling.html and whale.to/v/kalokerinos.html and [More information]
(4), (6) Trend and causes of neonatal mortality in the Kassena–Nankana district of northern Ghana, 1995–2002 Full Text
http://www.blackwell-synergy.com/links/doi/10.1111/j.1365-3156.2006.01582.x/full
(5) Vitamin A Working paper (John Snow, Inc.)
"It is fairly certain that the biggest change that has occurred in factors known to affect child mortality is the provision of vitamin A supplements to a large proportion of children in these regions." http://www.jsi.com/Managed/Docs/Publications/JSI_VitA_Working_Paper.pdf
(6) See (4)
(7) Rapid achievement of the child survival millennium development goal: evidence from the Navrongo experiment in Northern Ghana
http://www.blackwell-synergy.com/doi/abs/10.1111/j.1365-3156.2007.01826.x
(8) Accelerating reproductive and child health programme impact
http://www.realising-rights.org/docs/Navrongo%20experiment%20Ghana.pdf
(9) Ghana Accelerated Child Survival and Development approach (ACSD) [UNICF program]
http://www.unicef.org/evaluation/files/ghana.doc