Vaccination of Very Premature Infants
By
F. Edward Yazbak, MD, FAAP
The number of infants born prematurely has been steadily increasing in the United States. Very small and very premature infants are now surviving in increasing numbers.
The CDC has decided that in the majority of cases, infants born prematurely, regardless of birth weight, should be vaccinated with the same dose(s), at the same chronological age and according to the same schedule and precautions as full-term infants and children.
D’Angio et al of the Vaccine Research Unit at the University of Rochester have reported that during the first six months of life, extremely preterm infants mount lower antibody responses to vaccines than term infants.
Accordingly, the risks and benefits of the ever increasing number of mandated pediatric vaccines from birth to six months, need to be carefully re-examined for that specific group of infants.
------------------
When it comes to information about vaccines and vaccination research, it is becoming extremely difficult, even for professionals, to sort out the facts.
On March 6, 2007, a good friend in New Zealand who is well aware of my interest in MMR vaccination sent me a report originally filed by WMTW-TV Channel 8 in Auburn, Maine. The station is the ABC affiliate covering the greater Portland, ME area, a gorgeous part of New England, situated just three hours away by car from my home.
The title of the news item was
“Vaccines Safe For Preemies, Study Says –
MMR, Chicken Pox Shots Work In Pre-Term Infants
Vaccines for
measles-mumps-rubella and or chicken pox are effective
in extremely preterm infants, according to a new study
.
The rest of the news report read:
“ Pediatricians had assumed they would work, even though preemies' immune systems may not be fully developed.
"No one had formally researched the subject," said study author Dr. Carl D'Angio of the University of Rochester Medical Center. "I'm happy to be able to reassure my colleagues and parents that it is OK."
The study included 16 full-term and 16 extremely preterm infants born between May 2002 and May 2005. It examined the antibody levels of the diseases before and after vaccination. It was published in this month's issue of Pediatrics.
The same number of infants in each group reached a level considered protective.
"Now we can all breathe a sigh of relief. We were right," D'Angio said.”
It is entirely possible that an uninformed reader or young parent would interpret the above jubilant report as proving that the MMR and chickenpox vaccines were safe and effective in extremely preterm infants, like those often seen on television with breathing tubes and IV lines in incubators.
In fact, the infants who participated in the investigational study – all 32 of them - were healthy and 15 months old when they were vaccinated.
Relative to the safety statement, the infants were just seen twice, 3 to 6 weeks apart, and “safety” was assessed “by parental recall of vaccine-related adverse events and by active, prospective collection of blood-draw-associated adverse events”.
It should be noted that all MMR vaccine safety studies conducted by the vaccine industry have been notoriously short. Only two studies extended to eight weeks.
***
A
friend in Wales also sent me information about the same Rochester University
study that she had received via EurekAlert Science News Service.
http://www.eurekalert.org/pub_releases/2007-03/uorm-mcp030207.php
The tone of that news item was more restrained but its message was no less decisive.
“MMR, chicken pox vaccines work for preemies”
“Vaccines for measles-mumps-rubella and varicella, or chicken pox, are effective in extremely preterm infants, even though preemies' immune systems are not as developed as full-term babies. This confirms a long-held assumption by pediatricians and neonatologists across the country.”
"The assumption has always been that it would be OK, that very early babies would have enough immunity, but no one had formally researched the subject," said Carl D'Angio, M.D., associate professor of Pediatrics at the University of Rochester Medical Center, and author of a paper on the subject in Pediatrics this month. "I'm happy to be able to reassure my colleagues and parents that it is OK."
The Principal Investigator (PI) was again quoted as saying "Now we can all breathe a sigh of relief. We were right,"
According to the news report, the study was funded by the National Institute of Allergy and Infectious Diseases and the National Center for Research Resources of the National Institutes of Health.
***
The Official Study Record
![]()
MMR and Varicella Vaccine in Premature Infants
This study has been completed.
|
The
purpose of the study was listed as follows:
“This research is designed to address the question, “Does the relative deficit in vaccine immunogenicity in extremely premature infants persist beyond the first 6 months of life?”
Immunogenicity is the ability of a vaccine to provoke an immune response and result in immunity.
The above question, as stated, suggests that administration of one or several vaccines once, twice or three times to very small (< 1lb) and very premature (<28 wk gestation) infants during the first six months of life, does not provoke immune responses and therefore does not protect from illness. In a literal sense, all the administered antigens cannot be referred to as “immunizations”.
If that is so, then a true re-evaluation of risks and benefits of vaccinations administered in that population is in order and the statement by some that infants without exception have the capacity to respond to an enormous number of antigens (1) is invalid.
The PI goes on to describe the purpose of the study as follows:
“We propose to measure the immunogenicity of varicella and mumps-measles-rubella vaccines in relatively healthy, 12-to-15 month-old children born at <29 weeks gestation, when compared to full-term infants, as measured by the relevant viral serologies.”
In fact the enrolled infants were not “relatively” healthy. They had to be healthy.
Inclusion Criteria:
Subjects must meet all of the inclusion criteria to participate in this study.
1.
Premature infant < 29 weeks’ gestation at birth or term infant >/= 37 weeks’ gestation at birth. 2. Postnatal age < 16 months, 0 days. 3. Has not yet received MMR or varicella vaccines. (There are no restrictions on the administration of other vaccines at the time of MMR/varicella vaccination.) 4. Parental permission. 5. Agreement of primary care pediatrician/ health care provider. 6. Receives primary pediatric care within an approximate 25-mile radius of the University of Rochester. 7. Healthy status at enrollment. Exclusion Criteria:
1.
Known immunodeficiency. 2. Systemic corticosteroid therapy at the time of MMR/varicella vaccination. 3. Requiring oxygen therapy. 4. Clinically significant findings on review of medical history and physical exam determined by the investigator or sub-investigator to be sufficient for exclusion. 5. Any condition determined by the investigator that would interfere with the evaluation of the vaccine or be a potential health risk to the subject.
“Healthy status at enrollment”
According to the protocol “subjects will be approached at 9-12 months of age for inclusion”. They included sixteen ex-very premature infants had to be healthy, not only on the day they were vaccinated, but actually three to six months earlier, when they were registered. In other words, when the study was being conducted, those infants were the healthiest very small infants around Rochester, New York.
It should be pointed out that pediatricians are constantly told that they can and should vaccinate infants that are not in such pristine condition. Obeying such directives, pediatricians insist on vaccinating small preemies on oxygen and monitors, or who have colds and sniffles, on or close to schedule. Some actually threaten recalcitrant parents with referral to child protective agencies or exclusion from the practice.
The study
Study start: January 2004; Study completion: December 2005
Last follow-up: May 2005; Data entry closure: May 2005Title: MMR and Varicella Vaccine Responses in Extremely Premature Infants
“Phase: IV
Population: 16 generally healthy premature infants born at < 29 weeks’ gestation, < 16 months old from the Rochester area 16 generally healthy 37 weeks’ gestation,³full-term infants born at < 16 months old from the Rochester area
Number of Sites: University of Rochester
Study Duration: 1.5 – 8.5 months
Description of Agent or Intervention:
Subjects will make 2 study visits. The first, at 15 months of age, will coincide with a routine well child visit. Subjects will have 2 mL of blood drawn at the time of their routine, 15-month MMR, varicella, and pneumococcal conjugate immunizations. At a second study visit 4-6 weeks later, another 2 mL of blood will be drawn.
Objectives:
Primary: We propose to measure the immunogenicity of routinely administered varicella and mumps-measles-rubella vaccines in relatively healthy, 12-to-15 month-old children born at <29 weeks gestation (premature), when compared to that in full-term infants…
Safety will be assessed by parental recall of vaccine-related adverse events and by active, prospective collection of blood-draw-associated adverse events.
Schematic of Study Design:
Subjects will be approached at 9-12 months of age for inclusion, and will consent at this time or at Visit 1”
--------------
The study was
published in the March 2007 issue of PEDIATRICS.
(1)
A Medline abstract is available at http://tinyurl.com/36bfne
RESULTS: Preterm children had lower mumps and rubella geometric mean titers than did term children before vaccine, and nearly all children were seronegative for each of the 4 vaccine antigens before immunization. Measles, mumps, rubella, and varicella geometric mean titers were similar between groups after vaccine. All children were seropositive for measles after vaccine, whereas 13 of 14 preterm and 11 of 13 term children were seropositive for mumps, 13 of 14 preterm and 13 of 13 term children were seropositive for rubella, and 11 of 16 preterm and 9 of 15 term children were seropositive for varicella.
CONCLUSIONS: Preterm children mounted antibody responses that were similar to those of term children after measles-mumps-rubella and varicella vaccines at 15 months of age.
The CDC has long recommended the administration of the first dose of MMR and chickenpox vaccines at the age of one year and parents are cajoled and coerced to comply. This study does not guarantee that the risk taken by having 4 live attenuated virus vaccines administered simultaneously to small children is warranted. Indeed, as noted, even vaccination at 15 months of age did not result in full protection against rubella, mumps and chicken pox.
It is not clear why the investigators proposed to examine the immunogenic response between 12 and 15 months but actually waited to vaccinate the children until they were 15 to 16 months old. This is certain to raise questions.
The timing of the vaccinations brings out another indirectly related but yet very important point.
According to the American Academy of Pediatrics, the “routine” pediatric visit at which the MMR and chickenpox (and other) vaccines are administered should be scheduled at the age of twelve months. Why then was that “routine visit” actually “scheduled” at age 15 months in Rochester, the site of a major vaccine center?
--------------
The Principal
Investigator is a member of the Department of Pediatrics at the University of Rochester.
He is presently finishing a similar study on the pneumococcal
conjugate vaccine and is in the process of studying the influenza vaccine. All
32 infants in this study also received a dose of pneumococcal conjugate vaccine
at the age of 15 months.
The University of Rochester’s Vaccine Research Unit is renowned.
“The vaccine research effort at the University of Rochester Medical Center brings together a rare combination of resources that covers the gamut from basic research, to vaccine testing, to improving and measuring the availability of vaccines to people who need them most…. All vaccines depend on our knowledge of the basic workings of the immune system…
More recently, research done more than a decade ago by a trio of University virologists has become crucial to two promising vaccines designed to prevent cervical cancer. A vaccine to prevent this type of cancer, which kills more than 250,000 women around the globe every year, is expected to become available within a year, thanks in large part to technology developed at the University. The vaccine targets a group of viruses known as human papillomaviruses (HPV), which cause cervical cancer.
On the applied side, the University’s Vaccine and Treatment Evaluation Unit has had a hand in testing dozens of new vaccine candidates, including nearly every new vaccine to be approved in the last three decades. The unit is part of a network that the Federal government turns to for protecting the nation against infectious threats…
Just as important as creating or testing the vaccines, is getting them to the people who need them most. Here again, University doctors are part of virtually every large national network created to monitor the effectiveness of vaccines. The Rochester community finds itself one of the best vaccinated and best monitored in the world, and researchers worldwide have a grasp on just how well vaccines work, thanks to research by Rochester doctors.”
http://www.urmc.rochester.edu/pr/current_research/bird_flu/research.cfm
Funding for vaccine research at the University of Rochester Medical Center is provided by the National Institutes of Health and has almost doubled in five years (see graph).
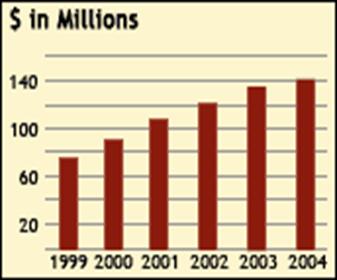
NIH Funding Continues to Grow at URMC
For parents in the autism community, the University of Rochester will
always be remembered as the place that produced the Pichichero Thimerosal study.
(2) Most of us are still scratching our heads about that study’s methodology and conclusions.
More recently, the University of Rochester Vaccine Research Unit offered to the world (and Merck coffers) the gift of the Human Papilloma Virus (HPV) vaccine.
See “How Cow Warts, Clergy Sex Surveys Moved Along Cancer Vaccine” at http://www.urmc.rochester.edu/pr/current_research/Cervical_Cancer_Vaccine/
“The creation of a successful vaccine against cervical cancer, approved today by the U.S. Food and Drug Administration, is the culmination of research that occurred thanks not only to scientists and physicians, but also to generous farmers and veterinarians, priests and nuns willing to tell all – and some very patient cows”(Thursday June 8, 2006)
On Tuesday February 8, 2007, the University of Rochester Medical Center published
“Preventing V.D. as Valentine’s Day Approaches”.
It started:
“With Valentine’s Day just around the corner, the world’s largest study of a vaccine to protect against genital herpes – a disease that infects approximately one of every four women and men in the nation – takes on special significance for Rochester-area women and their male companions.
Doctors and nurses are recruiting women in the Rochester area who don’t have genital herpes to help test a vaccine against the sexually transmitted disease. So far, 237 women locally have joined the study, making Rochester one of the lead sites nationally. But more female participants ages 18 to 30 are needed to effectively test the vaccine.”
The statement ended
“Men are not part of the study because previous studies have shown that the
vaccine does not work in men.”
That alone may have ruined the Valentine's Day in Rochester. http://www.urmc.rochester.edu/pr/news/story.cfm?id=1365
--------------
Discussion
All clinical trials of pediatric vaccines only enroll healthy infants and children and everyone makes certain that the infant or child is healthy at the time the vaccine is administered.
There are no studies where sick or “slightly sick” infants are vaccinated.
It is therefore strange that pediatricians are asked to vaccinate less than perfectly healthy infants and even stranger that they insist to do so.
In the recent Rochester study, the 16 ex-small preemies and the 16 normal infants used as controls received the MMR and chickenpox vaccines at the age of 15 months. In real life, the CDC recommends that these two vaccines be administered at 12 months of age when the ex-preemies are often more vulnerable.
“In the majority of cases, infants born prematurely, regardless of birth weight, should be vaccinated at the same chronological age and according to the same schedule and precautions as full-term infants and children. Birth weight and size are not factors in deciding whether to postpone routine vaccination of a clinically stable premature infant, except for hepatitis B vaccine. The full recommended dose of each vaccine should be used. Divided or reduced doses are not recommended”. (3)
In the case of live virus vaccines such as MMR, a follow-up period of 3 to 6 weeks is not long enough to evaluate safety.
One can only wonder why small very premature infants need the rubella, the mumps and the chickenpox vaccines at the age of twelve months.
Conclusions
The single most important conclusion that anyone can draw from “Measles-mumps-rubella and varicella vaccine responses in extremely preterm infants” is that extremely premature infants have a relative deficit in vaccine immunogenicity until the age of 6 months.
The issues that have been identified in this report will tend to compromise the significance of the study findings and their relevance to pediatric practice.
--------------
Footnote:
“The Rochester community finds itself one of the best vaccinated and best monitored in the world…”
http://www.urmc.rochester.edu/pr/current_research/bird_flu/research.cfm
The United States Congress passed the Children's Health Act of 2000 and mandated the establishment of centers of excellence in autism research. In response, the Institutes of the NIH Autism Coordinating Committee have implemented the STAART (Studies to Advance Autism Research and Treatment) network program.
One of the eight US Autism Research Centers of Excellence is located at the University of Rochester. Patricia Rodier, Ph.D., is the Director of the Center and Susan Hyman, M.D., FAAP is the Co-director.
According to Dr. Hyman, about 50% of Rochester area families with preschool children on the autistic spectrum use a gluten free and casein free diet. http://www.nimh.nih.gov/autismiacc/rochesterautism.cfm
References:
1. D'Angio CT, Boohene PA, Mowrer A, Audet S, Menegus MA, Schmid DS, Beeler JA. Measles-mumps-rubella and varicella vaccine responses in extremely preterm infants. Pediatrics. 2007 Mar;119(3):e574-9 2. Pichichero ME, Cernichiari E, Lopreiato J, Treanor J. Mercury concentrations and metabolism in infants receiving vaccines containing thiomersal: a descriptive study. Lancet. 2002 Nov 30;360(9347):1737-41. 3. Atkinson WL et al General Recommendations on Immunization CDC - MMWR February 8, 2002 / 51(RR02);1-36
F. Edward Yazbak, MD, FAAP
Falmouth, Massachusetts
© 2007